

Are Ancillary Services Missing In Rural Areas
Access to healthcare services is disquisitional to practiced health, yet rural residents face up a diverseness of access barriers. A 1993 National Academies report, Access to Healthcare in America, defined access as "the timely use of personal health services to attain the best possible health outcomes." A 2014 RUPRI Health Console report on rural healthcare admission summarizes boosted definitions of access with examples of measures that can be used to determine access.
Ideally, residents should be able to conveniently and confidently admission services such as primary intendance, dental care, behavioral health, emergency care, and public health services. According to Healthy People 2020, access to healthcare is important for:
- Overall physical, social, and mental health status
- Disease prevention
- Detection, diagnosis, and treatment of illness
- Quality of life
- Avoiding preventable deaths
- Life expectancy
Rural residents often come across barriers to healthcare that limit their ability to obtain the care they need. In order for rural residents to have sufficient access, necessary and appropriate healthcare services must be available and obtainable in a timely manner. Even when an adequate supply of healthcare services exists in the customs, there are other factors to consider in terms of healthcare admission. For case, to have practiced healthcare admission, a rural resident must also accept:
- Financial means to pay for services, such as wellness or dental insurance that is accepted past the provider
- Ways to accomplish and employ services, such as transportation to services that may be located at a distance, and the power to take paid time off of piece of work to employ such services
- Conviction in their ability to communicate with healthcare providers, particularly if the patient is not fluent in English language or has poor health literacy
- Trust that they can use services without compromising privacy
- Belief that they volition receive quality intendance
This guide provides an overview of healthcare access in rural America, including give-and-take on the importance and benefits of healthcare admission and the barriers that rural residents experience. The guide includes information on:
- Barriers to care, including workforce shortages and health insurance status
- Transportation
- Health literacy
- Stigma associated with weather condition in rural communities, such as mental wellness or substance abuse
For data on access to public wellness services in rural communities, run into the Rural Public Health Agencies topic guide.
Frequently Asked Questions
- How does the lack of healthcare access affect population health and patient well-being in a community?
- What are barriers to healthcare admission in rural areas?
- Why is master intendance access important for rural residents?
- What types of healthcare services are often difficult to access in rural areas?
- How exercise rural healthcare facility and service closures impact access to care?
- What are some strategies to improve access to care in rural communities?
- What can exist done to assistance rural veterans access healthcare?
- What is dissimilar almost healthcare admission for American Indians, Alaska Natives, and Native Hawaiians?
- What organizations work to meliorate rural healthcare access?
- How are private foundations working to improve healthcare admission and the related reimbursement issues?
How does the lack of healthcare access affect population wellness and patient well-being in a customs?
Co-ordinate to Access to Care: Populations in Counties with No FQHC, RHC, or Acute Care Infirmary, rural populations take more than limited access to primary care physicians than residents of urban areas, and are older, sicker, and poorer than urban counterparts. Travel to attain a chief care provider may be costly and burdensome for patients living in remote rural areas, with subspecialty care ofttimes beingness even further away. These patients may substitute local principal care providers for subspecialists or they may decide to postpone or forego care. Access in Cursory: Rural and Urban Health Care compares admission to care and utilize of services for rural and urban adults and children with Medicaid coverage.
Co-ordinate to the 2014 RUPRI Health Console report, Access to Rural Wellness Care - A Literature Review and New Synthesis, barriers to healthcare effect in unmet healthcare needs, including a lack of preventive and screening services and handling of illnesses. A vital rural community is dependent on the health of its population. While access to medical care does not guarantee good health, access to healthcare is critical for a population's well-being and optimal health.
The challenges that rural residents face in accessing healthcare services contribute to wellness disparities. To learn more about disparities in health outcomes, run across RHIhub'south Rural Wellness Disparities topic guide.
What are barriers to healthcare access in rural areas?
Distance and Transportation
Rural populations are more than likely to have to travel long distances to access healthcare services, particularly subspecialist services. This tin be a significant burden in terms of travel time, cost, and time away from the workplace. In improver, the lack of reliable transportation is a barrier to care. In urban areas, public transit is generally an option for patients to get to medical appointments; nonetheless, these transportation services are frequently defective in rural areas. Rural communities often accept more elderly residents who take chronic weather condition requiring multiple visits to outpatient healthcare facilities. This becomes challenging without available public or private transportation. RHIhub's Transportation to Back up Rural Healthcare topic guide provides resource and data about transportation and related problems for rural communities.
Workforce Shortages
Healthcare workforce shortages impact healthcare access in rural communities. One measure of healthcare access is having a regular source of intendance, which is dependent on having an adequate healthcare workforce. Some health services researchers argue that evaluating healthcare access by simply measuring provider availability is not an acceptable measure to fully sympathize healthcare admission. Measures of nonuse, such as counting rural residents who could not find an appropriate care provider, tin help provide a fuller picture of whether a sufficient healthcare workforce is available to rural residents.
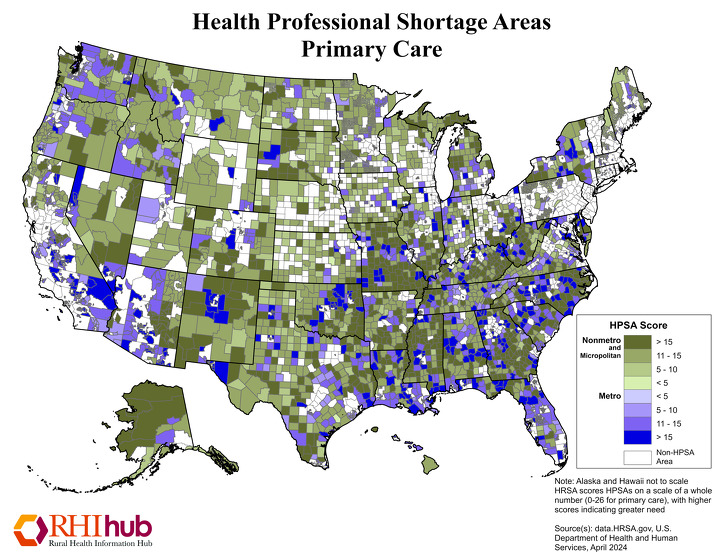
A shortage of healthcare professionals in rural areas of the U.S. tin can restrict access to healthcare past limiting the supply of bachelor services. As of March 2021, 61.47% of Principal Care Health Professional Shortage Areas (HPSAs) were located in rural areas. For the about current numbers, see HRSA's Designated Health Professional Shortage Areas Statistics.
Primary Care HPSAs are scored 0-25, with college scores indicating a greater need for primary care providers. This Nov 2021 map highlights nonmetropolitan areas with primary care workforce shortages, with areas in darker dark-green indicating higher nonmetro HPSA scores:
For more data on healthcare workforce challenges in rural areas, resource, and strategies used to address rural healthcare workforce shortages, run into RHIhub's Rural Healthcare Workforce topic guide.
Wellness Insurance Coverage
Individuals without health insurance accept less admission to healthcare services. A U.S. Census Bureau study, Health Insurance Coverage in the United states of america, 2018, plant that 9.ane% of the population living outside metropolitan statistical areas (MSAs) did non accept any blazon of health insurance in 2018, compared to 8.4% of the population within MSAs. Co-ordinate to Infants Without Wellness Insurance: Racial/Ethnic and Rural/Urban Disparities in Babe Households' Insurance Coverage, 2011-2015 data revealed that 19.ix% of infants in rural households did not accept health insurance, which was greater than the sixteen.viii% of infants in urban households who lacked insurance.
The June 2016 issue brief from the Part of the Assistant Secretary for Planning and Evaluation, Bear upon of the Affordable Care Human action Coverage Expansion on Rural and Urban Populations, constitute that 43.4% of uninsured rural residents reported not having a usual source of care, which was less than the 52.half-dozen% of uninsured urban residents reporting not having a usual source of care. The brief reports that 26.5% of uninsured rural residents delayed receiving healthcare in the past year due to price. The Affordable Care Act and Insurance Coverage in Rural Areas, a 2014 Kaiser Family Foundation effect cursory, points out that uninsured rural residents face greater difficulty accessing care due to the limited supply of rural healthcare providers who offer low-cost or charity healthcare, when compared to their urban counterparts.
Wellness insurance affordability is a concern for rural areas. A RUPRI Center for Rural Wellness Policy Assay policy brief, Wellness Insurance Marketplaces: Issuer Participation and Premium Trends in Rural Places, 2018, evaluated changes in average wellness insurance market (HIM) program premiums from 2014 to 2018. Average premiums were higher in rural counties than in urban counties. In addition, rural counties were more likely to have only 1 insurance issuer participating in the HIM.
Broadband Access
While the use of telehealth services was already condign more than popular and widespread at the kickoff of 2020, measures implemented in response to the COVID-19 pandemic accelerated this growth. Unfortunately, many areas lack access to broadband internet and experience tiresome internet speeds, both of which are barriers to accessing telehealth services. Compared to their urban counterparts, rural individuals are well-nigh two times more likely to lack broadband access. A Peterson Center on Healthcare and Kaiser Family unit Foundation written report, How Might Internet Connectivity Affect Wellness Care Access?, stated that vii% of people in metropolitan areas did not have access to internet at habitation in 2019, while 13% of people in nonmetropolitan areas lacked access. To larn virtually additional challenges for rural telehealth employ, see What are the challenges related to telehealth services in rural communities? on RHIhub's Telehealth Utilise in Rural Healthcare topic guide.
Poor Health Literacy
Health literacy tin also exist a barrier to accessing healthcare. Health literacy impacts a patient's ability to understand wellness information and instructions from their healthcare providers. This can be especially apropos in rural communities, where lower educational levels and higher incidence of poverty often impact residents. Low wellness literacy tin make residents reluctant to seek healthcare due to fearfulness or frustration related to communicating with a healthcare professional. Additionally, navigating the healthcare system tin be hard without health literacy skills. To learn more about low health literacy in rural America, see What are the roles of literacy, health literacy, and educational attainment in the health of rural residents? on RHIhub's Social Determinants of Health for Rural People topic guide. The Rural Monitor's two-role series on rural wellness literacy, Agreement Skills and Demands is Cardinal to Comeback and Who's Delivering Health Information?, explores connections between health and health literacy and how wellness information is being delivered to rural populations.
Social Stigma and Privacy Bug
In rural areas, because there is fiddling anonymity, social stigma and privacy concerns are more than likely to act as barriers to healthcare access. Rural residents can accept concerns almost seeking care for mental health, substance abuse, sexual wellness, pregnancy, or even common chronic illnesses due to unease or privacy concerns. Patients' feelings may be caused by personal relationships with their healthcare provider or others working in the healthcare facility. Additionally, patients can feel fear or concerns well-nigh other residents, who are ofttimes friends, family members, or co-workers, who may detect them utilizing services for wellness conditions that are typically not openly discussed, such as counseling or HIV testing services. Co-location or the integration of behavioral health services with primary care healthcare services in the aforementioned building tin can help ease patient concerns. Understanding Rural Communities, a 2018 podcast from the Hogg Foundation for Mental Health, features an interview with Dennis Mohatt, the Vice President for Behavioral Wellness at the Western Interstate Commission for Higher Education (WICHE), discussing rural health and the stigma surrounding mental healthcare in rural communities.
Why is master care access of import for rural residents?
Primary intendance is the most bones and, forth with emergency and public health services, the well-nigh vital service needed in rural communities. Master care providers offering a broad range of services and treat a wide spectrum of medical issues. The American Academy of Family Physicians characterizes primary care as follows:
"A primary care practise serves as the patient's first signal of entry into the health care system and equally the continuing focal point for all needed health care services…Master care practices provide health promotion, illness prevention, health maintenance, counseling, patient didactics, diagnosis and handling of acute and chronic illnesses in a diverseness of health care settings."
A 2005 Milbank Quarterly commodity, Contribution of Primary Care to Wellness Systems and Health, identifies the key roles primary care admission plays in preventing disease and improving health. Principal care serves as a showtime entry signal into the health system, which tin can exist particularly important for groups, such equally rural residents and racial/indigenous minorities, who might otherwise face barriers to accessing healthcare. Some benefits of principal care admission are:
- Preventive services, including early disease detection
- Care coordination
- Lower all-cause, cancer, and heart disease mortality rates
- Reduction in low nascence weight
- Improved wellness behaviors
Access to Quality Wellness Services in Rural Areas – Primary Care: A Literature Review, a section of the 2015 report Rural Healthy People 2020: A Companion Document to Good for you People 2020, Volume 1, provides an overview of the impact principal care admission has on rural health. Rural residents with express primary care access may non receive preventive screenings that can atomic number 82 to early detection and handling of illness. A North Carolina Rural Health Research Programme 2018 findings brief, Admission to Intendance: Populations in Counties with No FQHC, RHC, or Acute Care Infirmary, describes the scope of limited master intendance admission in rural areas in the U.South. and covers three facility types that provide primary care services to rural communities, including Federally Qualified Health Centers (FQHCs), Rural Health Clinics (RHCs), and acute care hospital outpatient departments. The findings brief found that in that location are 660,893 U.S. residents who alive in rural counties without an FQHC, RHC, or acute care infirmary. For more data on primary intendance in rural and urban areas, see Principal Care in the United States: A Chartbook of Facts and Statistics from the Robert Graham Middle.
To learn more about FQHCs, run across RHIhub's Federal Qualified Health Centers (FQHCs) topic guide. Additionally, RHIhub's Rural Health Clinics (RHCs) topic guide provides information and resources and answers oftentimes asked questions on these types of facilities.
What types of healthcare services are frequently difficult to admission in rural areas?
Dwelling Wellness
Home wellness services in rural America are a growing need. Abode is Where the Centre Is: Insights on the Coordination and Commitment of Domicile Health Services in Rural America, an Baronial 2017 Rural Health Reform Policy Research Heart policy brief, covers many barriers and challenges facing rural home health agencies that bear on their power to provide access in rural areas, including:
- Reimbursement and insurance coverage
- Face-to-face requirement
- Homebound status requirement
- Irresolute rules and regulations
- Workforce
- Time and resources required to serve patients located at a distance
- Belch process and referral difficulties
See To what extent are home health services bachelor in rural communities? on the Rural Habitation Health Services topic guide for more data.
Hospice and Palliative Care
Hospice and palliative care agencies oftentimes face up barriers and challenges similar to other healthcare services in rural areas. These challenges tin include workforce shortages; recruitment and retention programs; reimbursement bug; limited admission to broadband; and others.
RHIhub'south Rural Hospice and Palliative Care topic guide answers oftentimes asked questions and provides resource on hospice and palliative care in rural areas. Community-based Palliative Care: Scaling Access for Rural Populations, an October 2018 Rural Monitor article, describes the role palliative care plays in coming together the needs of patients who are chronically and seriously ill and covers challenges to accessing palliative care in rural areas.
Mental Health Services
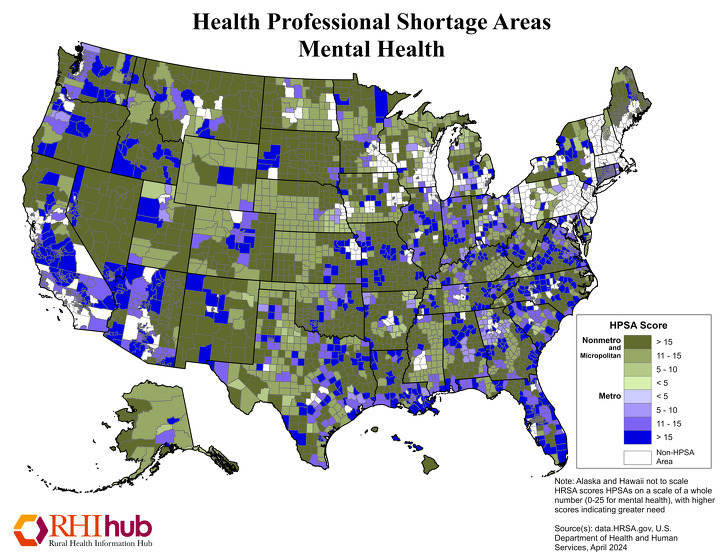
Access to mental health providers and services is a challenge in rural areas. As a event, master care physicians frequently make full the gap and provide mental health services while facing their own barriers, such every bit acceptable financial reimbursement or lack of time with patients. As of March 2021, 58.44% of Mental Health Professional Shortage Areas were located in rural areas. For the about current figures, see HRSA's Designated Wellness Professional Shortage Areas Statistics.
Mental Health HPSAs are scored 0-25, with higher scores indicating a greater need for mental health providers. The November 2021 map beneath highlights mental health HPSAs for both metro areas, in multiple shades of purple, and nonmetro areas, in diverse shades of light-green.
Due to the lack of mental health providers in rural communities, the employ of telehealth to deliver mental health services is on the rise. The June 2016 Agency for Healthcare Enquiry and Quality technical cursory, Telehealth: Mapping the Evidence for Patient Outcomes from Systematic Reviews, found that mental health services delivered via telehealth accept been shown to exist effective. By using telehealth commitment systems, mental health services can exist provided in a diverseness of rural settings, including rural clinics, schools, residential programs, and long-term care facilities. RHIhub'south Telehealth Employ in Rural Healthcare topic guide has many more resources on how telehealth can improve access to care. For additional resource on admission to mental health services in rural areas, see RHIhub'south Rural Mental Health topic guide.
For more than information, see the 2016 WWAMI Rural Wellness Research Heart data brief, Supply and Distribution of the Behavioral Health Workforce in Rural America. The brief discusses and compares the provider to population ratios of the behavioral health workforce in metropolitan and nonmetropolitan U.South. counties, including micropolitan and noncore areas. A land-level analysis of the study is also available with data for all states.
Substance Use Disorder Services
Despite a growing need, there is a definite lack of substance use disorder services offered in many rural communities across America.
A 2015 American Journal of Drug and Alcohol Abuse article, Rural Substance Use Treatment Centers in the U.s.: An Assessment of Treatment Quality by Location, reports that rural substance use disorder treatment centers had a lower proportion of highly educated counselors, compared to urban centers. Rural treatment centers were found to offer fewer wraparound services and specialized handling tracks.
Detoxification is an initial step of substance use disorder treatment that involves managing astute intoxication, withdrawal, and minimizing medical complications. A 2009 Maine Rural Wellness Research Center inquiry and policy cursory, Few and Far Away: Detoxification Services in Rural Areas, found that 82% of rural residents live in a county without a detox provider. The lack of detox providers in rural areas creates a barrier to care that could result in patients forgoing or delaying needed treatment. In lieu of a detox provider in a rural customs, the local emergency room or county jail, although non the nearly appropriate location for detoxification services, must ofttimes serve as a substitute.
Admission to medication-assisted treatment (MAT) is besides limited in rural communities. What's MAT Got to Do with It? Medication-Assisted Treatment for Opioid Utilise Disorder in Rural America provides an overview of MAT, an show-based treatment for opioid use disorder, with data on the scientific discipline behind the disorder and how 3 medications for opioid use disorder work.
A shortage of mental health and substance utilize disorder clinicians in rural communities led to the development of new models to span the gap and provide needed mental health and substance utilize disorder services using allied behavioral health workers, such as:
- Nurse Navigator and Recovery Specialist Outreach Plan
- ASPIN Network'due south Customs Health Worker Program
RHIhub's Substance Utilize and Misuse in Rural Areas topic guide provides information and resource, answers frequently asked questions, and lists model programs to accost substance employ disorder in rural areas.
Obstetric and Maternal Wellness Services
Closure of Hospital Obstetric Services Unduly Affects Less-Populated Rural Counties, an April 2017 policy brief from the University of Minnesota Rural Wellness Research Center (UMN RHRC), highlights the growing challenges women in rural areas face in accessing obstetric (OB) services. From 2004 to 2014, 179 rural counties lost hospital-based OB services, either to a infirmary or OB unit closure. Of the 179 rural counties losing OB services during that ten-year fourth dimension frame, 150 were noncore counties. A June 2020 UMN RHRC infographic, Loss of Infirmary-based Obstetric Services in Rural Counties in the United States, 2004-2018, displays like data. Co-ordinate to the certificate, only 27% of rural counties had hospital-based OB services equally of 2018. Additionally, a 2020 action plan from the U.S. Department of Health and Human Services, Salubrious Women, Good for you Pregnancies, Healthy Futures: Action Plan to Amend Maternal Health in America, points out that, although 15% of people in the U.Southward. live in rural communities, only 6% of OB/GYNs serve these areas.
A 2014 commission opinion from the American College of Obstetricians and Gynecologists (ACOG), Wellness Disparities in Rural Women, reports that "prenatal intendance initiation in the first trimester was lower for mothers in more than rural areas compared with suburban areas." Access to labor and delivery, prenatal, and related services is also a concern of ACOG, reporting that "less than one half of rural women live inside a 30-infinitesimal drive to the nearest hospital offering perinatal services."
A 2020 case report Making information technology Work: Models of Success in Rural Motherhood Care discusses iii rural obstetric service providers, highlighting the importance of strong partnerships, collaboration, and community back up to maintaining successful rural maternity care. The RHIhub Rural Maternal Health toolkit likewise discusses access to maternity care in rural areas.
The 2019 National Rural Wellness Association (NRHA) policy brief, Access to Rural Maternity Care, provides an overview of the decline in access to maternity intendance in rural areas and factors contributing to the turn down in access. The brief offers policy considerations to support maternity intendance services and accost barriers to access in the rural U.S., such as increasing research funding, rural OB practice challenges, workforce issues, and quality of OB care.
Oral Health Services
Oral health can affect overall physical and emotional health. For case, oral health needs that are not addressed can lead to pain, cosmetic concerns, and can affect academic or professional success. Despite the importance of oral wellness, access to dental care is either very limited or difficult to access in many rural and remote communities.
Traditionally, health insurance plans take non covered oral wellness services. A separate dental insurance program is needed to cover oral health services and procedures. A 2011 National Academies of Sciences, Engineering, and Medicine report, Advancing Oral Health in America, states that fewer rural residents have dental insurance compared to urban residents.
Another cistron limiting access to dental services is the lack of dental health professionals in rural and underserved areas. As of March 2021, 63.05% of Dental Health Professional person Shortage Areas were located in rural areas. For the almost current numbers, run across HRSA's Designated Health Professional person Shortage Areas Statistics. A June 2015 WWAMI Rural Health Research Center report, Dentist Supply, Dental Care Utilization, and Oral Wellness Among Rural and Urban U.S. Residents, found that rural adults used dental services less and had more permanent tooth loss compared to urban adults, which could be related to the scarcity of dentists in rural areas. The per capita supply of generalist dentists per 100,000 population, based on 2008 data, was xxx.1 for metropolitan areas, compared to 21.9 for nonmetropolitan areas.
A May 2018 NRHA policy brief, Improving Rural Oral Healthcare Access, offers recommendations to accost dental workforce shortages and to ultimately improve access to oral health services, including:
- Providing rural preparation tracks during dental education
- Albeit dental students from rural areas who would exist more likely to practice in a rural community
- Providing dental students opportunities to obtain a wide range of dental skills which will be needed in a rural practise
- Helping rural communities recruit and retain oral health providers through local community development programs
For more than information, come across What oral health disparities are present in rural America? on RHIhub's Oral Health in Rural Communities topic guide.
How do rural healthcare facility and service closures bear upon access to care?
The closure of rural healthcare facilities or the discontinuation of services can have a negative touch on on access to healthcare in rural communities.
Local rural healthcare systems are fragile; when 1 facility closes or a provider leaves, it can impact intendance and admission across the community. For example, if a surgeon leaves, C-section admission declines and obstetric care is jeopardized. If a hospital closes, it may be harder to recruit physicians.
There are multiple factors that can affect the severity and impact of a hospital or healthcare facility closure, including:
- Distance to the next closest provider
- Availability of culling services
- Transportation services
- Community members' socioeconomic and health status
Traveling to receive healthcare services places the burden on patients. For individuals with depression incomes, no paid fourth dimension off of their jobs, physical limitations, acute weather, or no personal transportation, these burdens can significantly affect their ability to admission healthcare services.
A significant concern for rural communities losing their hospital is the loss of emergency services. In emergency situations, any delay in intendance tin have serious adverse consequences on patient outcomes.
An 2015 findings brief from the North Carolina Rural Health Research Program, A Comparison of Airtight Rural Hospitals and Perceived Impact, identifies the following potential impacts on healthcare access due to infirmary closure:
- Unstable health services, particularly diagnostic and lab tests, obstetrics, rehabilitation, and emergency medical care
- Ascension Ems costs
- Residents not receiving needed care or services due to lack of transportation
- Greater impact on access for the elderly, racial/ethnic minorities, the poor, and people with disabilities
The North Carolina Rural Wellness Research Program maintains an interactive map, which displays locations of rural hospital closures in the U.S. from January 2005 to present. Co-ordinate to the map, 176 rural hospitals had closed as of December 2020. Unfortunately, rural health experts believe rural hospital closures are likely to keep because many rural hospitals accept minimal operating margins with piddling room for financial loss.
A 2016 Medicare Payment Informational Commission presentation, Improving Efficiency and Preserving Admission to Emergency Care in Rural Areas, describes policies and strategies to ensure access to emergency department services in rural areas. The presentation provides discussion on alternative healthcare delivery models. The 2020 research brief Alternatives to Infirmary Closure: Findings from a National Survey of CAH Executives explores options to maintain access in rural communities whose hospitals are encountering negative profit margins.
Maintaining chemist's shop services in rural towns can also be a claiming, especially when the only pharmacist in town nears retirement. When a community's only pharmacy closes, information technology creates a void and residents must adapt to find new ways to meet their medication needs. According to Causes and Consequences of Rural Pharmacy Closures: A Multi-Case Written report:
"Rural residents rely on local pharmacies to provide chemist's and clinical care direction and coordination. The absence of a chemist's shop may be unduly felt by the rural elderly, who often have a greater need for access to medications and medication management services."
A 2015 rural policy brief from RUPRI Center for Rural Health Policy Analysis, Characteristics of Rural Communities with a Sole, Independently Owned Chemist's shop, analyzed data to draw characteristics of vulnerable rural communities served by a sole, independently owned rural chemist's. Average characteristics of communities include:
- 19% of the population was aged 65 and older
- Unemployment at 8%
- Uninsured rates were 15%
- 28% had incomes beneath 150% of the federal poverty level
For more information on rural chemist's access or challenges rural pharmacies face, see RHIhub's Rural Pharmacy and Prescription Drugs topic guide.
What are some strategies to improve access to intendance in rural communities?
There are multiple strategies beingness used to improve access to healthcare in rural areas. Examples include:
Delivery Models
Freestanding Emergency Departments (FSEDs) are defined by the American College of Emergency Physicians (ACEP) equally a "facility that is structurally carve up and distinct from a infirmary and provides emergency intendance." ACEP provides FSED operational and staffing recommendations. A November 2016 Rural Monitor article, Freestanding Emergency Departments: An Alternative Model for Rural Communities, further defines a FSED and describes the ii types, while discussing the financial sustainability of the model. After Hospital Closure: Pursuing High Performance Rural Health Systems without Inpatient Intendance, a June 2017 RUPRI Health Panel report, discusses instance studies from 3 rural communities that transitioned to new models of care, including freestanding emergency section services, increased telemedicine chapters, and specialty care. The written report also describes a range of different commitment options for communities that lack hospital inpatient care.
In 2023, a new Medicare provider type will be implemented, the Rural Emergency Hospital, which is designed to maintain access to emergency and outpatient care in rural areas. For more information, see the RHIhub Rural Hospitals topic guide question What are Rural Emergency Hospitals?
Customs Paramedicine is a model of care where paramedics and emergency medical technicians (EMTs) operate in expanded roles to assist with healthcare services for those in need without duplicating available services existing inside the community. RHIhub'southward Community Paramedicine topic guide describes how this model of care tin benefit rural communities and covers steps to starting a rural customs paramedicine program. Rural communities looking to develop customs paramedicine or mobile integrated health programs tin also view RHIhub'south Rural Customs Paramedicine Toolkit for emerging practices and resources.
Frontier Community Wellness Integration Programme (FCHIP) is exploring the development of and testing new models to ameliorate access to quality healthcare services in frontier areas.
The Customs Health Worker (CHW) model facilitates healthcare access by using CHWs every bit a liaison between healthcare providers and rural residents to help make sure their healthcare needs are met. RHIhub's Community Health Workers in Rural Settings topic guide offers information and resources on CHWs and covers CHW teaching, training, and certification.
Team-based care models, such equally Patient-Centered Medical Homes (PCMHs), can also extend access to primary care services in rural communities. A multifariousness of rural medical abode and care coordination programs are highlighted in RHIhub'south Rural Wellness Models and Innovations section.
Amalgamation with Larger Systems or Networks
Local rural healthcare facilities may choose to bring together healthcare networks or affiliate themselves with larger healthcare systems as a strategic motility to maintain or improve healthcare access in their communities. These affiliations or joining of healthcare networks may improve the financial viability of the rural facility, provide additional resources and infrastructure for the facility, and allow the rural healthcare facility to offer new or expanded healthcare services they could not otherwise provide. Yet, the benefits of an amalgamation with a larger healthcare network may come at the expense of local control.
A 2018 RUPRI Middle for Rural Health Policy Assay policy cursory, Trends in Hospital System Affiliation, 2007-2016, notes that rural hospitals do follow the general trend and show an increase in infirmary system amalgamation. The brief found nonmetropolitan CAHs had the lowest rate of increase in infirmary arrangement amalgamation. The 2018 RUPRI Middle for Rural Health Policy Analysis report, The Rural Hospital and Health System Affiliation Landscape – A Cursory Review, discusses the various types of hospital affiliations that rural hospitals might consider and factors that might affect which option rural hospitals choose, such equally maintaining local decision-making authority and meeting the demands of the hospital system amalgamation. The written report covers some benefits infirmary organization affiliation tin beget a rural hospital, including admission to:
- Technology
- Staff recruitment and memory
- Group purchasing
- Increased access to healthcare and operational services
Efforts to Improve the Workforce
An adequate workforce is necessary to maintaining access to healthcare in a community. In order to increase access to healthcare, rural communities should exist using their healthcare professionals in the most efficient and strategic means. This might include allowing each professional to work at the top of their license, using new types of providers, working in interprofessional teams, and creative scheduling to offer clinic time exterior of regular work hours.
RHIhub's Rural Healthcare Workforce topic guide discusses how rural areas can address workforce shortages, such equally partnering with other healthcare facilities; increasing pay for staff; adding flexibility and incentives to improve recruitment and retentivity of healthcare providers; and using telehealth services. The guide also discusses land and federal policies and programs to improve the supply of rural health professionals, such as loan repayment programs and visa waivers.
Telehealth
Telehealth continues to be seen as a key tool to help accost rural healthcare access issues. Through telehealth, rural patients can meet specialists in a timely manner while staying in the condolement of their home or local facility. Local healthcare providers tin can also benefit from subspecialists' expertise provided via telehealth. Even so, the temporary changes to telehealth policy in response to the COVID-19 pandemic has made visible potential for unequal access to these services due to a lack of broadband net admission in some rural areas.
For more information on telehealth policy, including broadband capacity, see the Rural Policy Research Institute's 2020 report The Evolving Landscape of National Telehealth Policies during a Public Health Emergency: Responsiveness to Rural Needs. The written report notes the RUPRI Health Panel'due south recommendation that telehealth should support, not supplant local healthcare services.
RHIhub'southward Telehealth Use in Rural Healthcare topic guide provides a wide overview of how telehealth is existence used in rural communities to improve healthcare admission. The guide covers specific programs currently in use in rural areas, likewise every bit providing resource and a listing of funding and opportunities that tin be used to support telehealth solutions.
What tin can be done to help rural veterans access healthcare?
One of the primary barriers rural veterans face when accessing healthcare services is the meaning travel altitude to the nearest Veterans Affairs (VA) healthcare facility. A 2018 written report found that rural veterans' admission to healthcare is non necessarily an outcome of eligibility for purchased care from non-VA providers, as nearly VA healthcare facility deserts are also underserved by not-VA providers.
According to the 2019 enquiry brief Access to Care Among Rural Veterans, 56% of rural veterans enrolled in the VA health system are over 65 years of age and are more than likely to experience diabetes, middle conditions, and loftier blood force per unit area compared to urban veterans. Moreover, suicide rates are higher for rural compared to urban veterans.
To address admission issues for rural veterans, the VA has created community-based outpatient clinics in many rural areas, in addition to using mobile clinics and telehealth services. To larn more almost VA services for rural veterans or the VA'south efforts to address veterans' healthcare access, see RHIhub'southward Rural Veterans and Admission to Healthcare topic guide.
What is different about healthcare access for American Indians, Alaska Natives, and Native Hawaiians?
Health and Health Care for American Indians and Alaska Natives (AI/ANs), a 2018 publication from the Kaiser Family unit Foundation, reports that nonelderly AI/AN adults are more likely to be uninsured compared to nonelderly whites, 25% and 8% respectively, and that there are higher uninsured rates of AI/AN children (14%) compared to white children (4%). Health and Health Treat Asian Americans, Native Hawaiians and other Pacific Islanders (NHOPIs) in the United States, another 2018 publication from the Kaiser Family unit Foundation, found that eleven% of nonelderly Native Hawaiians and other Pacific Islander adults were uninsured in 2016 compared to seven% of nonelderly white adults.
The federal Indian Health Service (IHS) provides healthcare and prevention services to AI/ANs. Broken Promises: Continuing Federal Funding Shortfall for Native Americans, a 2018 report, reports that federal funding for Native American programs in the by 15 years has been severely inadequate and doesn't meet the bones needs and services of the federal government's obligations to the populations they serve, which in itself is a barrier to accessing healthcare for AI/ANs. IHS provides direct healthcare services at an IHS facility or Purchase/Referred Care (PRC) provided past a not-IHS facility or provider through a contractual agreement, and is not healthcare insurance coverage. This is explained further in RHIhub'south Rural Tribal Health topic guide question Is admission to Indian Health Service (IHS) resource considered health insurance?
RHIhub's Rural Tribal Wellness topic guide answers oftentimes asked questions on tribal health and provides resources on rural AI/ANs populations.
What organizations work to meliorate rural healthcare admission?
Many organizations work to meet the needs of rural communities and help ensure the availability of essential healthcare services.
- The Federal Role of Rural Health Policy (FORHP) focuses on rural healthcare issues and is function of HRSA.
- Rural Health Research Centers are funded by the Federal Function of Rural Health Policy to produce policy-relevant research and analysis on healthcare and problems impacting healthcare in rural areas.
- The National Rural Health Association (NRHA) provides leadership and resources on rural health bug for healthcare providers and organizations working to improve the health of rural communities.
- The National Association of Rural Health Clinics (NARHC) works to better the delivery of quality, cost-effective healthcare in rural underserved areas through the RHC Program.
- The American Infirmary Association (AHA) Section for Rural Wellness Services represents the interests of pocket-sized and rural hospitals and works to ensure that the unique needs of this segment of AHA'south membership are a national priority.
- State Offices of Rural Wellness (SORHs) and State Rural Health Associations help rural communities build healthcare delivery systems past analogous rural healthcare activities in the state, collecting and disseminating information, and providing technical assistance to public and non-profit entities.
- The National Organization of State Offices of Rural Health (NOSORH) works to foster and promote legislation, resources, and education with the SORHs, the Federal Office of Rural Wellness Policy, NRHA, and other organizations promoting and supporting rural healthcare access.
- The National Rural Recruitment and Retention Network (3RNET) is a national recruitment arrangement for healthcare professional jobs in rural and underserved communities.
How are private foundations working to improve healthcare access and the related reimbursement problems?
Many private foundations piece of work to ameliorate healthcare access by funding transportation services, improving workforce, and addressing other factors that affect rural healthcare access. Investing in existing safety net providers and programs, offer grants to develop and implement innovative healthcare delivery models, and funding research to study policy implications as they relate to rural healthcare access are all examples of deportment foundations can take to support rural healthcare admission.
A Nov 2017 article published in Health Diplomacy, Foundations' Efforts to Improve Rural Wellness Care, covers private foundation projects focused on improving access to rural healthcare.
Grantmakers in Health offers multiple resources that provide educational activity and guidance to foundations interested in improving rural healthcare access, such as Improving Health Care Access: Grantmakers Share Their Experiences or Improving Health Access in Communities, Lessons for Effective Grantmaking.

Source: https://www.ruralhealthinfo.org/topics/healthcare-access
Posted by: elzyowestrim.blogspot.com
0 Response to "Are Ancillary Services Missing In Rural Areas"
Post a Comment